Dr. Ahmad Shahzad
Founder | Lyallpur Diabetes Foundation
Consultant Diabetologist | Educator | Advocate for Preventive Care
Diabetics are more prone to foot complications, and diabetic foot infection is one of the most severe. The infections may arise when small cuts, blisters, or sores do not heal well because of poor circulation and nerve damage. Unattended, they can cause serious complications, such as ulcers or amputation. Educating about the reasons, early identification of the signs, and awareness of potential treatment available are crucial measures in preserving the health of the feet and general health.
What is a Diabetic Foot Infection?
A diabetic foot infection is a soft tissue or bone (below the ankle) infection in an individual with diabetes. It is common at the location of skin trauma or ulcers which is a common complication in diabetes, because of factors such as peripheral neuropathy, poor blood flow and immunity. Such infections may be mild on the skin and severe with deep tissue, abscesses and even bone infections (osteomyelitis). Aerobic gram-positive cocci, including Staphylococcus species (including methicillin-resistant Staphylococcus aureus (MRSA)) and in more severe cases polymicrobial, are known to cause diabetic foot infections. They cause lower extremity amputations in diabetic patients unless treated and managed.
Causes
Diabetic foot infections are multifactorial, and their causes are primarily linked to the underlying diabetic complications that affect the health and healing of the foot:
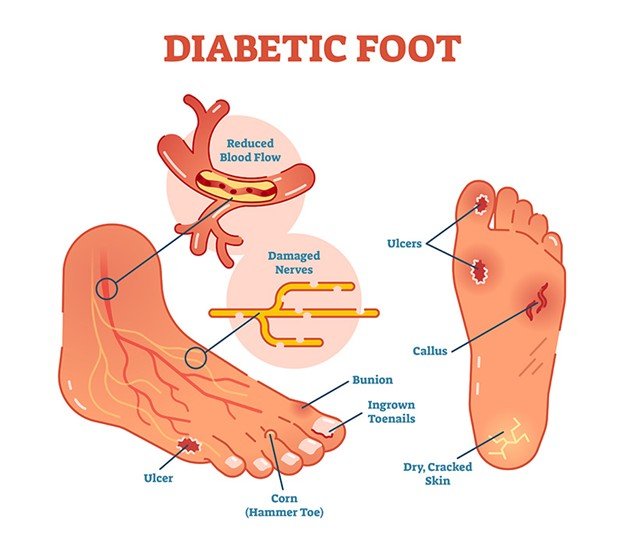
· Peripheral Neuropathy: Loss of sensation and autonomic nerve functions cause unperceived injury, dry skin, skin cracking, and foot deformities, which contribute to skin breakdown and infection.
Trauma, or Wounds: Foot trauma, ulcers, or wounds- caused by pressure, poor footwear, or repetitive injury. Penetrating wounds lasting longer than 30 days are at greater risk of infection.
· Peripheral Arterial Disease (PAD): This is the inability of blood to reach the tissues and provide oxygen and nutrients necessary to heal wounds and defend against infection.
· Poor Glycemic Control and Immunocompromised: High blood sugar (hyperglycemia) impairs the body to combat infection and slow healer.
· Other Factors: Smoking: Smoking leads to decreased blood flow, and delayed healing; foot deformities and calluses augment the number of pressure points; poor foot hygiene and improper nail care also elevate risk of infection.
All these predispose the diabetic foot to bacterial invasion and infection.
Symptoms
Diabetic foot infection has a variety of symptoms, which indicate infection, inflammation, and delayed healing. Symptoms to observe include:
- Skin changes and injuries: Cuts, sores, blisters, ulcers, or cracks on the feet that heal slowly, or slowly pus or fluid, with a bad smell.
- Redness, swelling, and warmth: Infected zones tend to be red, swollen, hot to touch, painful, but less painful in individuals with neuropathy.
- Discoloration: Skin discoloration around sores such as dark or black tissue which may be a sign of gangrene.
- Pain and numbness: Peripheral neuropathy develops pain, tingling, numbness, or loss of sensation, which can obscure signs of infections.
- Drainage: Yellow, green or smelly discharge around a wound or ulcer.
- Other signs: Shape of feet change, nail infection, loss of all hair on feet or legs, and in very serious cases, systemic, such as fever, chills, or extreme sickness in case of infection spread.
Early identification is essential to avoid development of severe infections, gangrene, or amputation.
Complications if Left Untreated
If left untreated, diabetic foot infections can lead to severe complications including:
· Transmission of infection: The infection may easily expand to the deeper structures of muscle, tendons, and bones (osteomyelitis) complicating the treatment and recovery of the infection.
· Gangrene: Tissues may die (gangrene) due to severe infection and inadequate blood circulation, a medical emergency that can require urgent surgery.
· Amputation: Untreated infections may cause partial or total amputation of toes, foot, or even lower leg to avoid the further spread of infection and save the life of the patient.
· Sepsis and systemic disease: Infection can be introduced into the blood and lead to sepsis. It is a life-threatening disease with systemic inflammation and organ dysfunction.
· Types of chronic wounds: Chronic non-healing ulcers carry risks of repeated infections and disability.
· Low-quality life: The pain, loss of mobility, prolonged stay in the hospital, and even loss of a limb affects the overall wellbeing and independence of patients.
These risks should be minimized by early diagnosis and treatment. It avoid long-term morbidity and mortality among patients with diabetic foot infection.
Diagnosis of Diabetic Foot Infections

Diabetic foot infection diagnosis requires a mixture of clinical evaluation and diagnostic tests:
- Clinical Examination: Diagnosis is mostly clinical, through demonstration of local infection, like redness, warmth, swelling, pain / tenderness, and purulent discharge. Depth and exposure of bone are evaluated by careful inspection following cleaning and debridement.
- Classification: The extent and systemic signs are used to classify the severity. In terms of the Infectious Diseases Society of America (IDSA) or International Working Group on the Diabetic Foot (IWGDF) as uninfected, mild, moderate, or severe infection.
- Probe-to-Bone Test: This is a simple test in which a sterile metal probe is applied to determine whether bone is palpable. It indicates osteomyelitis (bone infection). It is sensitive and specific and relies on operator expertise.
Imaging:
- Small-pox X-rays to identify the presence of bone or foreign bodies.
- MRI is indicated to diagnose osteomyelitis when there is inconclusive clinical evidence.
- Other imaging modalities such as PET, SPECT, or CT can be used in complicated cases.
Laboratory Tests:
- Blood tests such as complete blood count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) are used in diagnosis and evaluating inflammation.
- Blood cultures when there is a suspicion of systemic infection.
- Biopsy of deep wound or tissue samples to culture microbiological culture to identify causative pathogens and antibiotic therapy (superficial swabs are less reliable).
Other: Assessment of peripheral arterial disease, neuropathy, and overall health status is also essential in diagnosis and planning treatment.
Treatment Options
Management of diabetic foot infections (DFIs) mainly includes a combination of antibiotic treatment, wound care, and occasionally surgery. The practice relies on the severity of the infection, complications, and patient factors:
Antibiotic Therapy
- Mild infections: Oral antibiotics are applied that are directed toward common Gram-positive bacteria. MRSA coverage is commonly covered with cephalexin, dicloxacillin or trimethoprim-sulfamethoxazole in case of necessity.
- Moderate to severe infections: need broader-spectrum antibiotics that are usually intravenous, including Gram-positive, Gram-negative, anaerobes, and resistant bacteria, such as MRSA and Pseudomonas aeruginosa. They include vancomycin and piperacillin-tazobactam, cefepime, carbapenems or combinations based on culture findings.
- Typical duration is 1-2 weeks in mild cases but may last up to 3-4 weeks or longer in case of severe infections or slow to resolve infections or osteomyelitis. Step-down therapy is usually oral following initial IV therapy.
Wound Care
- Debridement and drainage of abscesses.
- Frequent dressing and cleaning to keep the wound wet.
- Unloading of the affected foot to help healing.
Surgical Treatment
- Indicated in patients who have gangrene, necrotizing fasciitis, or gangrene.
- Surgical denial of infected or necrotic tissue can be done.
- Severe or refractory cases may require limb salvage operation or amputation.
- To enhance blood circulation and healing, vascular interventions may be discussed in patients with peripheral arterial disease.
Supportive Measures
- Optimization of glycemic control.
- Management of comorbidities like peripheral arterial disease and neuropathy.
- Patient education to prevent recurrence and promote foot care.
You may also like to read: Importance of Foot Care in Diabetes Management
Prevention of Diabetic Foot Infections
The prevention of diabetic foot infections includes maintenance of foot health, early detection of issues, and risk factors. Major prevention measures are:
- Foot inspection and hygiene: Routinely examine feet to look for cuts, blisters, redness, swelling or wounds with a mirror or a helper (caregiver). Clean feet with tepid water every day, dry (with special care between them), and put between toes to avoid cracks and dryness, but do not apply moisturizer.
- Footwear: Wear well-fitting shoes, with adequate toe space, cushioning and support. Wear no tight or rough-edged or ill-fitting shoes, sandals or walking barefoot, even in the house. Diabetic shoes and pads can prevent pressure ulcers.
- Nail and skin care: trim toenails straight and file ends in order to avoid ingrown nails. Do not self-treat corn and calluses; contact a professional. Peel off calluses.
- Consistent check-up of the feet: Frequent foot examinations by medical practitioners to detect early issues and particularly in high-risk patients with neuropathy or peripheral arterial disease.
- Treat underlying conditions: Good glycemic control, cessation of smoking, exercise, and treatment of peripheral arterial disease enhance circulation and nerve condition, lowering the risk.
- Education and early treatment: Educate patients about foot care and seek medical attention to any abnormalities on the feet to avoid further development of an infection.
Such actions, can significantly decrease the risk of foot ulcers and follow-up infections among diabetic individuals.
Final Thoughts
Infection of diabetic foot infection is a severe problem. It must be treated well and immediately. Identifying the red flags, controlling blood sugar levels, and proper foot care help people with diabetes to significantly decrease their risk. Early diagnosis and timely treatment effectively preclude complications, as well as safeguarding long-term health and mobility. Foot care is one of the most useful precautions to maintain health and safety with diabetes.