Dr. Ahmad Shahzad
Founder | Lyallpur Diabetes Foundation
Consultant Diabetologist | Educator | Advocate for Preventive Care
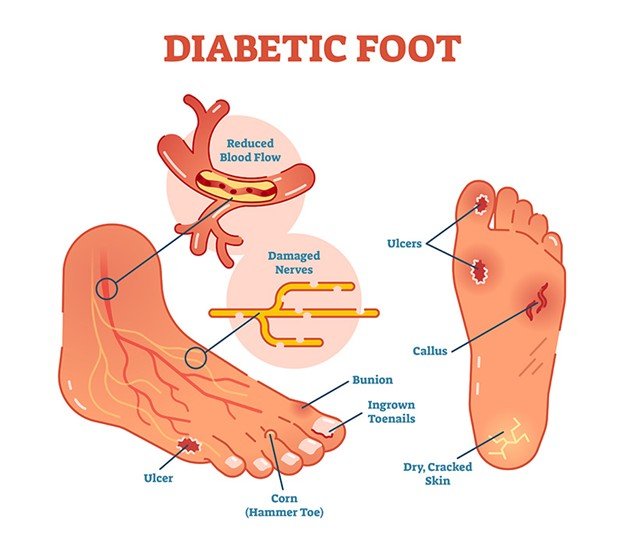
One of the most severe diabetes complications, diabetic foot ulcers. It usually result in infection, hospitalization, and even amputation without appropriate treatment. Treatment is critical to ensure healing, prevent complications, and enhance life quality. This article examines the various management methods of diabetic foot ulcers and the results that patients can attain when managed well.
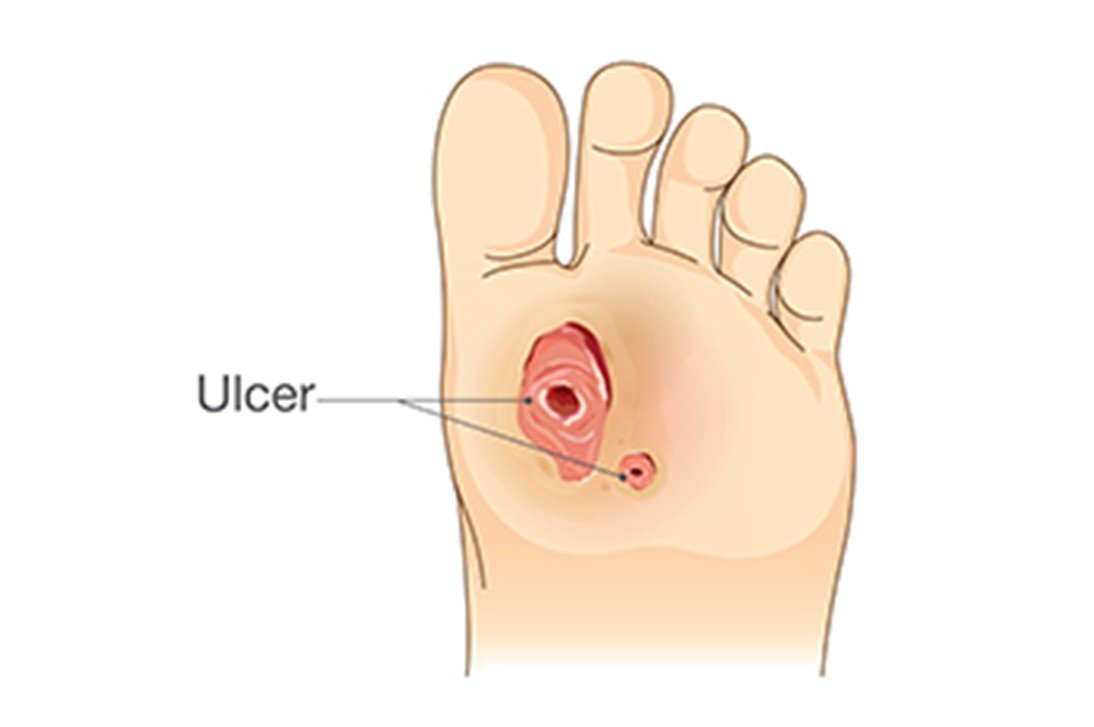
Understanding Diabetic Foot Ulcers
DFUs are open wounds or ulcers that usually develop on the lower part of the foot in diabetic patients. They ocurr due to diabetes complications like peripheral neuropathy (nerve damage), lack of circulation (ischemia), and infection. These ulcers are severe as they raise the susceptibility of infections. It may result in hospitalization, amputation and severe health complication without treatment.
Conventional Treatment Options
Traditional medication therapies of diabetic foot ulcers (DFUs) are primarily aimed at managing multifactorial etiology. It facilitat wound recovery by various means:
Offloading
- Offloading the ulcer site to debride pressure is the most urgent intervention. The gold standard is the nonremovable total-contact cast (TCC) that redistributes plantar pressure and allows the foot to rest but not do much.
- Other components can be half-shoes, rigid-soled postoperative shoes or accommodative dressing.
Wound Debridement
· Frequent cleansing of skin tissue (debridement) is required to heal and to prevent the development of infection.
Infection Control
· Systemic and topical antibiotics are applied in the case of infection, particularly in cellulitis or osteomyelitis.
Wound Dressings
· A wet wound environment is to be maintained. The wound is covered by conventional dressings and by highly developed wound care products that absorb exudate and stimulate healing.
Revascularization
· Wound healing potential may require interventions to enhance the circulation with vascular surgery or angioplasty as in the case of patients with poor blood flow.
Adjunctive Therapies (often add-ons to conventional care)
Growth factors include platelet-derived growth factor (PDGF).
· Negative pressure wound therapy (NPWT) maximizing blood flow and removing exudate.
· Hyperbaric oxygen therapy to enhance oxygen supply to tissues.
Growth factors include platelet-derived growth factor (PDGF).
· Negative pressure wound therapy (NPWT) maximizing blood flow and removing exudate.
· Hyperbaric oxygen therapy to enhance oxygen supply to tissues.
Multidisciplinary Care
· An interdisciplinary model that incorporates endocrinologists, podiatrists, vascular surgeons, infectious disease, and wound care nurses has been proven to provide much better results, reducing the risk of amputations and accelerating recovery.
Advanced and Surgical Treatments

Surgical and advanced treatment of diabetic foot ulcers (DFUs) offer an alternative to standard care, particularly in case of severe, nonhealing, or complicated ulcers.
Advanced Treatments
- Platelet-Rich Plasma and Fibrin Therapies: Platelet-rich plasma or fibrin patches can be used to facilitate wound healing by increasing tissue regeneration and the delivery of growth factors.
- Topical Oxygen Therapy (TOT): TOT proves to be much more effective in chronic DFU healing than hyperbaric oxygen therapy, which demonstrates limited efficacy, because of its ability to deliver oxygen to tissues topically.
- Negative Pressure Wound Therapy (NPWT): It involves controlled suction to clear out exudate, edema, and enhances blood circulation, which helps complex wounds to heal.
- Regenerating Agents (RGTAs): These are synthetic natural extracellular matrix components that protect proteins, induce new tissue development and inhibit inflammation.
- Bioengineered Skin Substitutes and Nanotechnology: Assists in supporting tissue regeneration, infection control and providing growth factors or antimicrobials to promote healing.
- Digital Health Technologies: AI-wound assessment and telemedicine are new means of streamlining the process of personalizing treatment and follow-up.
Surgical Treatments
- Debridement: This is the surgical debridement of dead or infected tissue to support healing and prevent infection; this may involve multiple surgeries.
- Abscess Drainage: To prevent the spread, incision and drainage of localized infections.
- Bone Surgery: Bone is removed or shaved to decrease pressure points and risk of infection; deformities may be corrected (hammertoes, bunions, or Charcot foot).
- Revascularization Surgery: Arterial bypass or angioplasty to reestablish blood flow to patients with peripheral arterial disease, which improves wound healing.
- Skin Grafts and Flaps: These are applied on persistent or large ulcers to cover and heal the wound, thus preventing infection by bacteria.
- Amputations: Only done when there is severe infection or tissue necrosis that threatens life or limb and has minimized amputation.
- Joint Alignment/Fusion, Tendon Lengthening: Right biomechanical defects involved in ulcer development or healing.
You may also like to read: Preventing Diabetic Foot Ulcers
Outcomes of Treatment
The history of diabetic foot ulcer (DFU) management is quite diverse and depends on the severity of the ulcer, infection, blood circulation, time frame, and general health status of the patient.
Healing Rates and Prognosis
· Approximately 44-50% of infected DFUs recover fully after 12 months of conventional and multidisciplinary care. Recovery can be 78% at 1 year with interdisciplinary teams in special centers.
· At 4 weeks, a 41.8% decrease in wound size is a predictor of improved healing at 3 months.
· Recurrence rates are high, with about 10 percent of patients who heal develop new ulcers in one year.
Amputations and Surgical Outcomes
· DFUs have a lower extremity amputation (LEA) of 17-47% incidence. Approximately half of admitted DFU patients had surgical debridement and almost half received LEA as first line treatment in some cohorts.
· Minor amputations (e.g., toe disarticulations) occur more frequently than major amputations (e.g., below-knee or above-knee).
· Revision surgery is common because of persistent infection or failure of wound to heal, with reports of up to 30-40% in studies.
Mortality and Morbidity
- Mortality one year post presenting with an infected DFU may be up to 15 percent—greater than many standard cancers in some series–and such severe systemic effects of DFUs and related infection.
- Morbidity such as long hospitalization (2-3 weeks or more) and reduced quality of life are frequent.
Factors Affecting Outcomes
Multidisciplinary care and wound centers enhance healing and amputation
· Poor glycemic control, infection severity, ischemia, and neuropathy aggravate prognosis.
· Early treatment, no multiple ulcers, good blood flow (perfusion), and reduced duration of ulcers are all related to better results.
Final Thoughts
The management of diabetic foot ulcers involves a mix of prompt medical attention, enhanced treatment solutions, and self-management. After attentive wound healing, blood sugar management, and prevention, patients can significantly enhance outcomes and decrease the risk of severe complications. Preventive care and suitable treatment are the only way to keep feet healthy and well.