Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
Maintaining general health depends on sleep, but for diabetics it is even more so. Studies demonstrate that bad sleep might impair blood sugar regulation, insulin sensitivity, and energy levels, hence complicating condition management. Knowing how sleep and diabetes are related helps to illuminate why regular, quiet sleep is not just a luxury but also a crucial component of diabetes treatment and prevention.
Understanding the Link Between Sleep and Diabetes
Bad sleep raises the risk of getting diabetes, but diabetes can interfere with sleep—thus establishing a two-way connection. Insufficient or too much sleep hurts blood sugar regulation by altering hormones, aggravating insulin resistance, and hence supporting weight gain. Conversely, symptoms of diabetes like frequent urination or neuropathy-induced pain can disturb sleep.
How poor sleep increases diabetes risk
Lack of sleep can throw hormones that control stress (like cortisol) and hunger (like ghrelin) off balance, therefore impairing blood sugar management.
Sleep deprivation causes the body to be less efficient at utilizing insulin, hence raising insulin resistance, a major precursor to type 2 diabetes.
Weight gain: Bad sleep may cause increased hunger and weight gain, both of which raise the risk of developing type 2 diabetes.
Unhealthy habits: Tiredness from a lack of sleep can lead to poorer dietary choices and less physical activity, further increasing diabetes risk.
How diabetes disrupts sleep
Regular urination (nocturia): Increased blood sugar can wake you awake often to urinate.
Pain and discomfort: Diabetic neuropathy can cause pain, tingling, or burning in the feet and hands, making it difficult to sleep soundly.
Nocturnal hypoglycemia: Low blood sugar levels during the night can cause sweating, nightmares, or confusion upon waking.
Many individuals with diabetes also have sleep apnea, hence there is a clear correlation between the illness and diabetes.
Benefits of Restful Sleep for Diabetic Health
Restful sleep promotes diabetic health by bettering blood sugar control, balancing hormones including insulin and cortisol, and aiding weight management. It helps the body to utilize insulin more effectively and lowers the risk of developing insulin resistance, therefore lowering blood sugar levels. and the beginning of diabetes type 2.
Key benefits of restful sleep for diabetic health
Better blood sugar control: Proper sleep helps maintain more steady blood sugar levels and enhances the body’s management of blood sugar following meals. Higher morning blood glucose levels can result from not getting enough sleep.
Sleep controls important hormones including insulin, ghrelin (a hunger hormone), and cortisol (a stress hormone). Poor sleep can upset this balance, resulting in high cortisol levels that cause the liver to release more glucose and thereby raise blood glucose.
When well-rested, your body is better at using insulin to transport glucose from the blood into cells for energy. Lack of sleep might raise insulin resistance, thereby complicating your body’s control of blood sugar.
Sleep helps to control appetite hormones, so a lack of it can cause more hunger and snacking. Controlling diabetes depends on maintaining a healthy weight.
Encouragement of mental and physical activity: Good sleep is necessary for general physical and mental health; hence, it helps your body to operate normally in everyday life.
Tips to Improve Sleep Quality for People with Diabetes
By selecting low glycemic foods and tracking glucose levels—particularly preventing nighttime hypoglycemia—manage blood sugar fluctuations.
Steer clear of stimulants and caffeinated beverages few hours prior bedtime.
To help with blood sugar control and lower stress, participate in consistent physical exercise, especially earlier in the day.
Create a regular bedtime ritual and sleep schedule even on weekends.
Before bed, limit blue light from electronic devices; perhaps read a book instead.
Since alcohol interferes with deep sleep cycles, stay away from it before bed.
Set the bedroom quiet, dark, and cool to make it sleep-friendly.
Control stress with relaxation approaches like mild yoga or meditation.
If sleep disorders are possible, think about talking with a healthcare provider; treatments like CPAP or sleep aids could be necessary.
These techniques promote better blood glucose management and general diabetes control by enhancing the quality and length of sleep.
Final Thoughts
In conclusion, maintaining healthy sleep habits is an essential part of managing and preventing diabetes. Restful sleep supports stable blood sugar levels, improves insulin function, and enhances overall well-being. By prioritizing quality sleep and addressing any underlying sleep issues, individuals with diabetes can take an important step toward better health and a more balanced lifestyle.
FAQs
How many hours of sleep do diabetics need?
Diabetics should seek for 7 to 9 hours of excellent sleep each night, equal to that of the general adult population. Too much sleep as well as too little might impair blood sugar regulation by influencing insulin sensitivity and other metabolic mechanisms. Controlling blood sugar depends on having a consistent sleep schedule and following good sleep hygiene.
What does diabetic fatigue feel like?
Diabetes tiredness manifests itself as intense and unrelenting exhaustion, continual lack of energy, cognitive haze, and general weakness not cured by rest or sleep. Often caused by the body’s inability to utilize insulin to change glucose into energy, which results in exhaustion, and may also come from High or low blood sugar levels cause irritability, slowness, and inability to focus.
Is too much sleep bad for diabetes?
Other sleep disruptions and disorders, such as sleep apnea, also seem to raise a person’s odds of having diabetes. But the risk goes up at the other end of the spectrum, too. For reasons that aren’t clear, people who sleep too much — more than 9 hours a night — might also have higher chances of getting diabetes.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
Exercise is vital for diabetes management because it helps to regulate blood sugar, boost insulin sensitivity, and improve general health. Incorporating exercise into everyday life will greatly benefit the mental as well as physical health of diabetics. Still, one should keep in mind that not all exercises fit all people and that certain safety precautions have to be taken. This essay examines the main benefits of exercise for diabetics together with crucial safety precautions to bear in mind while beginning a successful fitness program.
Understanding the Connection Between Exercise and Diabetes
While high-intensity exercises like weightlifting or sprinting can momentarily raise blood sugar, aerobic activity normally lowers it. Long-term benefits of consistent physical activity also exist. Advantages include improved well-being, decreased heart disease risk, and better weight control.
How exercise helps
Enhance insulin sensitivity: Consistent exercise makes your cells more reactive to insulin, hence enabling them to use glucose more efficiently and decrease blood sugar.
Manages blood glucose: Active muscles consume glucose for energy, therefore preventing its buildup in your circulation.
Helps with weight control: Exercise supports weight reduction or maintenance, which is a major factor in diabetes management.
Lowers other risks: It lowers stroke and heart disease risk, regulates blood pressure and cholesterol, and enhances general health.
Types of exercise and their effects
Aerobic exercise: Low, ongoing activities such walking, swimming, cycling, or running helps to lower blood sugar.
High-intensity activity, that is, workouts with short bursts of strong motion like sprinting, high-intensity interval training (HIIT), or weightlifting—can briefly elevate blood sugar levels. because stress hormones were released.
Stretching: Depending on the circumstances, light stretching may not greatly affect blood sugar levels.
Key tips for exercising with diabetes
Always check your blood sugar before, during, and after activity to see how your body reacts to various stimuli.
Watch for hypoglycemia (low blood sugar): Exercise burns glucose, which might reduce your blood sugar. This is a specific danger for people using insulin or specific diabetes drugs.
Stay hydrated and eat a little snack or fruit to avoid hypoglycemia should your blood sugar be under your target prior exercise.
If your blood or urine test reveals ketones, stay away from hard activity. Call your physician.
Plan your exercise; usually 1 to 3 hours after a meal—when blood sugar levels are naturally higher—is the best time to work out.
Always consult your doctor before beginning a new workout routine, especially if you take drugs. They can assist you to adapt. your insulin or medicines dosage as required.
People with diabetes can obtain several advantages from exercise, including weight management, better insulin sensitivity, and better blood glucose management. Improving cardiovascular health, lowering blood pressure, and raising mood and general well-being will also help to reduce complications. Consistency is crucial, and especially successful for diabetes control is the mix of aerobic and strength training.
Blood glucose control and insulin sensitivity
Exercise helps your cells grow more sensitive to insulin so that it can better reduce blood glucose levels.
Controls blood sugar: Regular exercise helps your body to process glucose and lowers blood glucose during and after a workout.
Muscle mass created by strength training improves insulin sensitivity and helps control blood sugar.
Cardiovascular health
Enhancing Heart Health: Aerobic activities such walking, swimming, and cycling are good for cardiovascular health.
Reduces stroke and cardiac disease risk: Particularly crucial for people with diabetes, regular exercise helps to decrease stroke and heart disease risk.
Aids in weight management: Exercise is a crucial part of managing your weight.
Boosts mood: Physical activity can lead to an improved mood and overall sense of well-being.
Reduces injury risk: Flexibility and balance exercises, such as yoga, can help reduce the risk of injury.
Important considerations
Especially for people on medication, a regular exercise program is essential for controlling blood sugar; consistency is crucial.
Because some workouts might lower or raise blood glucose levels, it is advised to test your blood sugar before, during, and after exercise.
Consult a physician: Speaking with your healthcare provider is crucial before you begin or modify your exercise regimen.
Common Mistakes to Avoid
Common mistakes include ignoring blood sugar levels and neglecting to bring quick-acting carbohydrates, exercising in extreme temperatures, not consulting a doctor, and ignoring pain or potential injuries, especially to the feet. It is crucial to monitor blood sugar, stay hydrated, listen to your body, and choose appropriate exercises based on individual health conditions.
Final Thoughts
Regular exercise is one of the most efficient means to control diabetes and enhance long-term health. People with diabetes can safely experience the many physical and emotional advantages of being active by selecting appropriate activities, keeping track of blood sugar levels, and taking needed precautions. Regularity and adequate direction can turn exercise into a strong ally in better blood sugar management, more energy, and general healthier lifestyle.
FAQs
How to exercise safely with diabetes?
The most prudent strategy is to frequently check your blood sugar. Before working out, measure your blood glucose. Check it as well during workout if you are working out for more than 45 minutes, especially if this is an exercise you have not done regularly. Both immediately after exercise and then later, verify your blood sugar level.
What is the 15 minute rule for diabetes?
If your blood sugar is low, eat 15 grams of carbs then wait 15 minutes, following the 15-15 rule. Recheck your blood sugar. Repeat this procedure if it is still under 70 mg/dL.
What is the best time to exercise for diabetes?
For those with prediabetes or type 2 diabetes, for instance, timing exercise to follow meals could have advantages; but people with type Earlier in the day, exercising might help with 1 diabetes.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
Prompt identification and proper therapy of ketoacidosis, a major metabolic illness, are essential. Adherence of evidence-based ketoacidosis recommendations guarantees correct diagnosis, successful treatment, and better patient outcomes. From evaluating severity and starting treatment to avoiding recurrence, these criteria define important actions for healthcare practitioners to help guarantee patient safety and recovery.
Understanding Ketoacidosis
Serious condition ketoacidosis develops when the body, lacking insulin, converts fat for energy, therefore generating excessive amounts of acids called The most prevalent in people with type 1 diabetes, ketones accumulate in the blood.
How ketoacidosis develops
The body requires insulin to transport glucose (sugar) from the blood into cells for energy.
In the absence of sufficient insulin, the body begins to break down fat for energy as glucose cannot be employed.
Acidic byproducts known as ketones result from ketone production.
Buildup happens when ketone synthesis is excessively rapid; they accumulate in the blood and urine, thereby causing the blood to become extremely acidic.
Common causes and triggers
Mostly a result of type 1 diabetes, but can also happen in type 2.
New onset diabetes: Ketoacidosis can show itself on first diagnosis.
Infection: A diabetic emergency can result when illness causes the body to require extra insulin.
One of the most frequent causes is not taking insulin as directed; non-adherence with treatment.
Other causes: A significant risk factor is high blood sugar levels over (250) mg/dL.
Signs and symptoms
High blood glucose (hyperglycemia)
Nausea, vomiting, or abdominal pain
Dry mouth and increased thirst
Frequent urination
Fruity-smelling breath (due to acetone)
Tiredness and weakness
Confusion or difficulty paying attention
Rapid, deep breathing (Kussmaul respiration)
Treatment Guidelines
Treatment guidelines for ketoacidosis mostly emphasize insulin therapy, fluid and electrolyte replacement, and addressing underlying causes such as infection. Critical phases include first intravenous (IV) fluid restoration, next intravenous insulin to address hyperglycemia and ketosis, then monitoring and replacing electrolytes, particularly potassium.
Usually, 0.9% normal saline, isotonic fluids help hypovolemia correction, restore tissue perfusion, and clear ketones by means of fast first hydration.
Fluid deficits could be as great as 10–15 percent of body weight.
Following the first hydration, electrolytes and sodium levels may determine adjustments of fluids.
Insulin Therapy
The typical treatment is continuous intravenous insulin infusion, with doses usually at 0.1 U/kg/h; however, 0.14 U/kg/h without an initial bolus is also effective.
Only when potassium is confirmed to be higher than 3.3 mmol/L is insulin infusion started.
Dextrose is added to IV fluids and insulin dose is changed if plasma glucose drops to 200–250 mg/dL but ketoacidosis remains.
For minor or uncomplicated DKA outside of intensive care unit environments, subcutaneous insulin regimens might be applied.
Electrolyte Replacement
Despite normal or elevated serum potassium initially, total body potassium deficiency demands potassium replacement.
Insulin treatment risks hypokalemia by changing potassium intracellularly.
If potassium is less than 3.3 mmol/L, insulin is postponed; potassium supplementation comes first.
Usually sufficient unless kidney failure is present, potassium is maintained between 4-5 mEq/L with 20-30 mEq per liter of IV fluids supplementation.
Monitoring and Resolution Criteria
Regular blood glucose, electrolyte, pH, bicarbonate, anion gap, and clinical status monitoring is required.
Resolution is defined by blood glucose below 200 mg/dL plus two of the following: serum bicarbonate over 15 mEq/L, venous pH over 7.3, or anion gap less than 12 mEq/L.
Once ketoacidosis clears and the patient can tolerate oral intake, conversion to subcutaneous insulin can be carried out.
Final Thoughts
Adherence to established ketoacidosis guidelines is crucial for prompt action and best patient care. Healthcare professionals may lower problems and increase recovery outcomes by adhering to appropriate diagnostic methods, treatment plans, and preventive measures. Preventing further occurrences and guaranteeing patient safety depend mostly on ongoing education and awareness.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
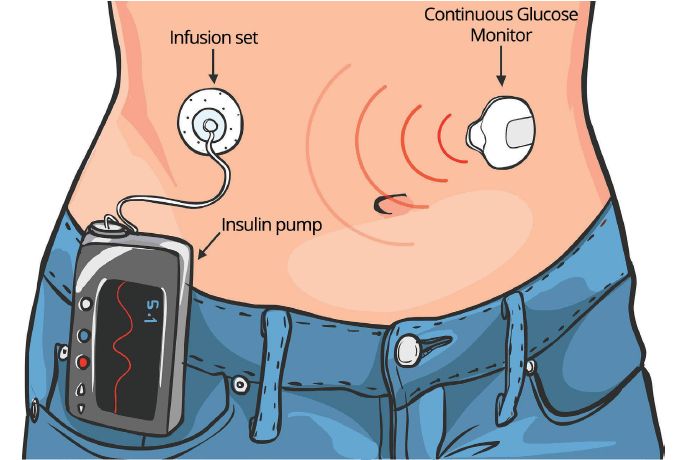
Good diabetes management calls for tight control of blood glucose levels; therefore, insulin distribution helps greatly in attaining that balance. Often known as insulin pump therapy, continuous subcutaneous insulin infusion (CSII) has become a sophisticated treatment that closely mimics the natural release of insulin. CSII provides better flexibility, accuracy, and comfort for people living with diabetes—particularly those who trying to keep regular glucose levels with conventional injections.
What is Continuous Subcutaneous Insulin Infusion (CSII)?
Through the skin (subcutaneous tissue), Continuous Subcutaneous Insulin Infusion (CSII) employs a tiny, portable, battery-powered pump to distribute insulin. Providing a constant background (basal) rate of insulin with additional doses (boluses) given for meals, it is meant to replicate the body’s own insulin release. Compared to several daily injections, this strategy provides more flexibility and better glycemic control.
How it works
Usually, on the abdomen, a cannula is inserted under the skin and linked to an infusion set via a little, wearable pump.
The pump is set to constantly provide a regular, low dose of insulin (basal rate) during both day and night.
The pump can also be manually programmed by the user to administer a greater insulin dose (bolus) to help with meals.
Modern hybrid closed-loop systems may interact with a continuous glucose monitoring sensor to automatically modify the basal rate.
Benefits of Continuous Subcutaneous Insulin Infusion
Closely reproduces the way the pancreas releases insulin naturally.
According to the National Institutes of Health (NIH) and Springer, studies demonstrate better glycemic profile and lower HbA1c may result from improved blood glucose regulation.
More freedom in meal timing and daily activities is provided by greater flexibility.
How CSII Differs from Traditional Insulin Therapy
In its delivery method, insulin kind, and flexibility, continuous subcutaneous insulin infusion (CSII), or insulin pump treatment, sets itself apart from conventional insulin therapy—multiple daily injections (MDI). CSII employs one type of rapid-acting insulin given continuously via a pump and catheter unlike MDI, which combines numerous daily injections of long- and quick-acting insulin.
Key differences between CSII and MDI
Feature
Continuous Subcutaneous Insulin Infusion (CSII)
Multiple Daily Injections (MDI)
Delivery method
An automated pump delivers insulin continuously through a small catheter placed under the skin. The pump provides a continuous trickle of insulin (basal rate), which the user can program to vary throughout the day.
Injections are manually administered using syringes or insulin pens. This method involves injecting long-acting insulin (basal) one to two times per day and rapid-acting insulin (bolus) with each meal.
Mimics physiological insulin
CSII more closely mimics a healthy pancreas by providing a steady supply of insulin tailored to an individual’s specific needs. This can result in less fluctuation in blood glucose levels.
This method attempts to mimic the body’s normal insulin production but is less precise and flexible than CSII. The duration of long-acting insulin and timing of meals are crucial to this process.
Flexibility
Offers greater flexibility with meals, exercise, and daily routines. Users can easily adjust basal rates for activities or sickness and deliver extra insulin (bolus) for meals on demand.
Requires a more rigid schedule. Insulin injections and meals must be timed consistently, which offers less flexibility in day-to-day life.
Hypoglycemia risk
Can potentially lower the risk of severe hypoglycemia, as the pump can be programmed to suspend insulin delivery if glucose levels drop too low.
Severe hypoglycemic events may be more frequent when compared to CSII, especially in those with frequent blood sugar lows.
Glycemic control
Can lead to better overall glycemic control, with studies often showing a lower HbA1c and better time-in-range for CSII users, especially in patients with suboptimal control on MDI.
Offers good glycemic control for many but can be less effective for those with highly variable blood glucose levels.
Patient commitment
Requires a high level of motivation, education, and commitment from the patient. Users must constantly manage the device, including changing the infusion set every few days and monitoring glucose levels frequently.
Also requires commitment to a strict schedule, but the daily tasks are generally less demanding than managing a pump. However, dosing errors can have serious consequences.
Cost and convenience
Has a higher upfront cost for the pump, plus ongoing expenses for supplies like reservoirs and infusion sets. The pump is a continuous device that must be worn almost constantly.
Involves lower initial costs, and ongoing expenses are limited to insulin vials/pens and needles. Some individuals prefer not to wear a device and prefer injections.
Potential Risks and Limitations
Possible dangers of Continuous Subcutaneous Insulin Infusion (CSII) are metabolic problems such as diabetic ketoacidosis (DKA) from pump failure or set issues and skin Problems, including lipohypertrophy at the infusion site, infection, and irritation. Limitations include the risk of weight gain, the inconvenience for activities such as sports or showering, and the possibility of patient-related problems such as adverse psychological effects and user error.
Practical suggestions for Continuous Subcutaneous Insulin Infusion (CSII) users include regular rotations of insertion sites, adequate understanding of often monitoring blood glucose levels, your pump’s configurations, and a backup plan for pump breakdown. Always keep rapid-acting carbohydrates available, understand how to manage hypoglycemia, and check in often with your medical team.
Site management and hygiene
Before replacing an infusion set, wash your hands thoroughly with soap and water.
More frequently, if the site becomes inflamed, switch your infusion set every 2 to 3 days.
To prevent irritation and guarantee even absorption, turn your infusion sites. Although the thigh or hip can also be used, the stomach is a frequently used and good area.
Get ready to contact a doctor if you see symptoms of infection, like hardness, redness, or discomfort by preparing the new collection on a clean surface.
Pump management and safety
Keep track of your baseline rates, insulin-to-carb ratios, and correction factors in case you have to go back to manual injections.
Get to know your pump’s alerts and what they signify. Keep in mind that the pump might not alert for a failed location that stops giving insulin.
Never separate the pump for longer than an hour without a different insulin supply to prevent diabetic ketoacidosis (DKA).
Shield the pump from strong radiation and electromagnetic fields, as this can damage the device.
Blood sugar monitoring and treatment
To avoid ketosis, monitor your blood glucose levels four times a day at least.
Before altering your pump settings, always address a low blood sugar (hypoglycemia).
Always have fast-acting carbs for treating hypoglycemia.
Include how to give glucagon or glucogel if necessary when sharing knowledge on how to treat a hypo with relatives or friends.
Patient and caregiver collaboration
Include the user of the pump in their own diabetes management since they know their own body and have the expertise on their own condition.
Ensure your healthcare staff is familiar with CSII technology and that you can communicate effectively with them.
Final Thoughts
A contemporary, adaptable, and exact way of treating diabetes is constant subcutaneous insulin infusion. It helps people reach better glucose management and higher quality of life by offering constant insulin delivery and adjustable dosing. Although CSII calls for adequate education, consistent monitoring, and dedication, its advantages typically outweigh the difficulties for those looking for a more natural and efficient means to control diabetes.
FAQs
What is the 3 hour rule for insulin?
Rapid-acting insulin (also known as Insulin Stacking) starts working around 15 minutes after injection, reaches its peak in about one hour, and Still works 2 to 4 hours. The three-hour restriction avoids “insulin stacking” and low blood glucose (BG) or hypoglycaemia.
Does CGM have a needle?
Does a CGM contain needles? Your CGMs’ accompanying CGM applicator has a little needle used to install the gadget to the rear of your arm. Once in place, a little filament linked to the sensor stays under your skin so the gadget can determine your glucose levels using interstitial fluid.
Which insulin is best for diabetes?
Long-acting or intermediate-acting insulin
Once or twice daily, this kind of insulin is taken. They might advise a kind of long-acting insulin (brand names Levemir, Lantus, Toujeo, Tresiba, If you either have frequent low blood sugar (hypoglycemia, or hypos), Semglee or Abasaglar.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
Worldwide, diabetes is among the top causes of renal failure; when kidney function deteriorates significantly, dialysis offers a crucial treatment choice. Dialysis and diabetes’s relationship emphasizes how long-term elevated blood sugar damages the kidneys, resulting in chronic kidney disease. For diabetic patients to maintain general health and enhance quality of life, it is imperative to know the process of dialysis, its many forms, and how to successfully treat both diseases.
What Is Diabetes and How Does It Affect the Kidneys?
Diabetes is a disorder characterized by the body having too much blood sugar (glucose) brought on by either insufficient or ineffective insulin. By impairing the fragile filtering system of the kidneys, diabetic nephropathy—a disease—it can damage them. Over time, this damage can lead to chronic kidney disease (CKD) and eventually, kidney failure.
How diabetes affects the kidneys
Kidneys have millions of little filters known as nephrons that purify the blood. High blood sugar can harm these nephrons as well as their blood vessels.
Weak filtration: Damaged blood vessels and nephrons cannot correctly filter excess fluid and waste from the blood.
One of the consequences of the injury is damage to the filters, which causes them to begin leaking and lets beneficial protein escape into the urine. Early indicators of kidney damage.
Accumulation of waste: As kidney function degrades, poisonous substances and waste products collect in the blood.
Diabetes sometimes causes high blood pressure, which adds extra strain on and damage to the kidneys.
If uncontrolled, this escalating damage can cause end-stage renal disease (ESRD), wherein the kidneys shut down completely. Dialysis or a kidney transplant are both possibilities here.
When Does a Diabetic Patient Need Dialysis?
Usually, in stage 5 of chronic kidney disease (CKD), when their kidneys have progressed to end-stage renal disease (ESRD), a diabetic patient needs dialysis. When the kidneys are operating at only 10–15% of their usual ability. At this point, the kidneys can no longer efficiently filter waste from the blood; dialysis or a kidney transplant is therefore required to support life. Usually, following a period in which kidney damage from high blood sugar has grown severe, resulting in symptoms like high blood pressure, swelling, and foamy urine, this phase is frequently preceded by one.
Types of Dialysis for Diabetic Patients
The two main forms of dialysis for diabetic patients are peritoneal dialysis, which filters blood outside the body using an artificial kidney, and hemodialysis (HD). (PD), which filter the blood using the abdominal lining. Although both treatments are effective renal replacement for end-stage kidney disease, their usefulness can vary on personal patient requirements and medical factors.
Hemodialysis (HD)
Blood is extracted from the body, filtered by an artificial kidney (dialyzer) to get rid of waste and excess fluid, and then sent back to the body.
Access: Calls for a surgical operation to establish permanent access, like an arteriovenous fistula or graft. Initially, one can utilize temporary catheters.
Involves frequent in-center treatments that could result in blood-borne illness exposure and cardiovascular strain.
Peritoneal dialysis (PD)
An acting filter, dialysis solution is introduced into the peritoneal cavity, which is the lining of the abdomen. Then the solution with waste products is drained out.
Access entails surgically inserting a permanent abdominal catheter.
Includes automated peritoneal dialysis (APD) and continuous ambulatory peritoneal dialysis (CAPD), both of which employ a machine at night.
Considerations: Provides more flexibility for at-home treatment, could protect residual renal function, and could help to better manage blood pressure. It presents hazards, including hyperinsulinemia, central obesity, and dyslipidemia.
Dialysis diabetes management calls for a thorough strategy including frequent blood sugar monitoring, a deliberately designed kidney-friendly diet, and consistent drug administration. Managing blood sugar variations and safe fluid intake requires close collaboration with a healthcare team, including a dietitian, to modify drugs and diet. Light exercise can also be beneficial; therefore, you should inform your dialysis staff of any changes in blood sugar results.
Dietary management
Working with a dietitian is necessary to design a meal plan that harmonizes your kidney health and diabetes.
Aim for three balanced meals a day, with nutritious snacks if necessary to stop blood sugar from falling too low or rising too high.
Select low-potassium foods: Concentrate on low-potassium fruits and vegetables like cabbage and apples.
Limit specific foods: Stay away from sugary beverages, fried meals, and meals heavy in salt or processed carbohydrates.
Choose sugar-free substitutes in meals and baking.
Medication and monitoring
Regularly check your blood sugar and talk with your care team about healthy ranges.
Adhere to a regular timetable; even on days for dialysis, take your meds as directed. Particularly for insulin, your care team could modify the timing or amount to accommodate dialysis sessions.
Pay particular attention to modifications in insulin doses: On the day of dialysis, physicians could have to lower insulin doses, especially basal insulin.
Medications should be discussed with your physician since their effect on kidney function can call for changes or substitutions of some oral diabetes drugs. One might think about oral medications with a reduced hypoglycemia risk.
Report unexpected readings: Whether they are too high or too low, let your dialysis staff know of any strange blood sugar levels.
Lifestyle and other health factors
Keep active: Walk or stretch as authorized by your medical staff to help regulate blood sugar and enhance circulation by means of light, safe activities.
Manage fluid intake: Since this is crucial on dialysis, adhere to the advice of your care team.
Be mindful of hypoglycemia, or low blood sugar, particularly if your appetite is poor or you have nausea. For those undergoing dialysis, this presents a greater risk.
Monitor other factors: Regular examinations for heart and blood vessel disease are crucial, given that it is a frequent consequence for patients with both kidney and diabetes.
Bottom Line
Early diagnosis, good blood sugar management, and consistent medical attention emphasize the link between diabetes and dialysis. Effective diabetes control is still essential in preventing extra issues, even if dialysis helps to replace some kidney capabilities. Following a balanced diet, keeping track of glucose levels, and closely consulting with medical professionals help patients enhance their well-being and live a more healthful life. A more steady life despite the difficulties of both situations.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
A balanced diet is absolutely crucial for diabetes control and maintenance of overall health. Because diabetes affects the metabolism of glucose in the body, prudent food choices are essential to keep blood glucose levels inside of a normal range. Maintaining the right proportions of carbohydrates, proteins, fats, and fiber may help control glucose fluctuations, maintain energy levels, and prevent problems. When individuals understand how food helps to manage diabetes, they can make informed decisions supporting long-term stability and health.
Understanding Diabetes and Its Dietary Connection
Diabetes is a disease marked by high blood sugar brought on by the failure of the body to produce or use insulin effectively. Controlling it depends on a nutritious diet, and the link is great: diets rich in nuts, fruits, vegetables, and whole grains can help to prevent diabetes Although risk rises for individuals high in processed meats, sweet beverages, and refined grains, With meals cooked at consistent intervals, a nutritious diabetes diet emphasizes nutrient-dense, high-fiber foods.
Key aspects of a diabetes-friendly diet
Concentrate on complete foods; eat plenty of fruits, veggies, and whole grains.
Choose good fats from nuts, seeds, avocados, and olive oil rather than saturated fats from red meats, processed meats, and some oils.
Limit particular foods: Lower intake of refined grains, sugar-sweetened drinks (including fruit juices), and sweet treats like cookies and cakes.
High-fiber foods are what you should aim for since they help to control blood glucose levels. Often advised is a target of at least 14 grams of fiber per 1,000 calories.
Stay hydrated; instead of sugary drinks, consume lots of sugar-free beverages or water.
Be aware of protein sources such beans, nuts, eggs, and lean meats, but restrict processed and red meats because of correlations with other health issues.
Watch your serving sizes to keep a healthy weight.
Keep standard eating times: Eating at fixed intervals can help control blood sugar levels.
The Importance of a Balanced Diet for Diabetics
Diabetics need a balanced diet to regulate blood sugar, lose weight, and lower their risk of problems, including heart disease. Eating consistent meals with a mix of high-fiber carbohydrates, lean protein, and good fats is one part of this process; another is controlling portion sizes and being careful of carbs. Intake: To develop a customized diet based on personal needs, one should see a licensed dietitian.
Why a balanced diet is important
Maintaining blood sugar (glucose) levels within a safe range, a balanced diet helps to avoid both high blood sugar (hyperglycemia) and the long-term Among other problems it can bring on are nerve, cardiac, and renal damage.
Healthy eating—particularly when coupled with weight loss—can help to control blood sugar levels and offers further health advantages.
Reduced chance of complications: A balanced diet aids in control of heart disease risk factors including high blood pressure and elevated blood fats.
Better general health: Adequate nutrition enhances mood, raises energy levels, and stimulates the body’s antioxidant activity.
The Role of Meal Planning and Portion Control
Controlling diabetes depends on meal planning and serving size control since they help to stabilize blood sugar levels, maintain a healthy weight, and avoid complications. While portion control prevents overeating and guarantees steady carbohydrate intake and improved overall nutrient intake, a meal plan offers direction for well-balanced, consistent meals.
Meal planning for diabetes
Create a customized plan reflecting your objectives, preferences, and way of living in collaboration with a healthcare practitioner or registered dietitian.
Emphasize balanced meals: Each meal should have a combination of healthy fats, lean protein, and complex carbs to encourage hunger and keep blood sugar stable.
Choose foods heavy in nutrients: Emphasize non-starchy vegetables, whole grains, and lean proteins like fish, beans, or chicken. Reduce added sugars, processed foods, and fine grains.
Distribute meals and snacks: Having little, well-balanced meals every few hours helps to maintain steady blood sugar levels.
Portion control for diabetes
Know usual serving amounts, such as half a cup of cooked pasta or a 3-ounce serving of meat, that of a deck of cards.
Especially when beginning out, precisely measure food using measuring cups, spoons, or a kitchen scale.
Try the Plate Method: one-quarter should be lean protein, one-quarter should be complex carbohydrates such as whole grains, and half should be non-starchy veggies.
Extras include sauces, condiments, and even certain oils, adding extra calories, sugar, or fat. Check nutritional information and limit their use.
Popular Dietary Approaches for Diabetes
Among common dietary strategies for diabetes are the plate approach, which emphasizes balanced meals of non-starchy veggies, lean protein, and carbohydrates; carb counting, which entails keeping tabs on carbohydrates; Specific dietary patterns like the Mediterranean or MIND diets as well as carbohydrate consumption to control blood glucose levels. Emphasizing entire foods and regulating eating windows to handle insulin resistance, plant-based diets and sporadic fasting are other often used alternatives.
The Plate Method: A simple visual guide to meal planning.
Fill half your plate with non-starchy vegetables (e.g., broccoli, spinach, green beans).
Fill a quarter with lean protein (e.g., fish, chicken, beans, tofu).
Fill the final quarter with a carbohydrate (e.g., whole grains, starchy vegetables like peas).
Carbohydrate Counting: A method for more precise blood sugar management.
Track and limit the total number of carbohydrates eaten at each meal.
Work with a healthcare provider or dietitian to determine your target carb amount.
Mediterranean and MIND Diets: These patterns combine elements of the Mediterranean diet with other healthy eating styles.
Include vegetables, nuts, olive oil, whole grains, berries, and fish.
Focus on whole foods and limit added sugars and refined carbohydrates.
Plant-Based Diets (Vegan/Vegetarian): Focus on foods from plants.
Rich in fiber and antioxidants, with lower saturated fat content.
Eliminates all animal products, including meat, fish, and dairy.
Intermittent Fasting: Involves alternating between periods of eating and fasting.
It can help manage insulin resistance and other diabetes-related factors.
Work with a healthcare provider to ensure safety, especially if you take certain medications.
Final Thoughts
Diet, in the last analysis, is among the most effective instruments for diabetes management. By stressing balanced nutrition, portion control, and mindful eating, people may help to keep their blood sugar stable and lower their chance of complications. Combining a nutritious diet with consistent physical exercise and expert direction guarantees a long-lasting strategy to diabetes control and general improved quality of life.
FAQs
How does diet contribute to diabetes?
Diets high in processed carbohydrates have been connected to a higher risk of developing type 2 diabetes. Foods rich in saturated fats: You might not associate diabetes with saturated fats, but this bad dietary fat has been connected to insulin resistance.
What is the best diet for insulin resistance?
Emphasizing veggies, fruits, and whole grains while restricting processed foods, sugary beverages, and bad fats, the ideal diet for insulin resistance centers on whole, unprocessed foods. Important ingredients include lean proteins from sources such as fish and chicken, high-fiber foods including beans, lentils, and berries, and beneficial fats from sources like almonds, seeds, and olive oil. Managing blood sugar and increasing insulin sensitivity are made possible by limiting processed snacks, red meat, and white bread.
Does rice spike blood sugar?
Because rice is a high-carbohydrate food that is readily digested and turned to glucose, spike in blood sugar can especially occur with white rice. The kind of rice, serving size, and other foods consumed with it will all influence the degree of the spike. Rice’s digestion and blood sugar response can be slowed by combining it with fiber, protein, healthy fats.
Is roti good for diabetes?
Yes, because of its reduced glycemic index and increased fiber, roti made from whole wheat or other whole grains is normally beneficial for diabetes. than white rice, which manages blood sugar. It’s crucial to eat it in small amounts, though, and to stay away from processed flours (maida), which can cause blood sugar peaks.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
The monitoring of blood glucose (SMBG) is a crucial aspect of successful diabetes management. It enables patients to monitor their own blood sugar levels, enabling them to learn how their diet, physical activity, stress, and medications affect their blood sugar levels. Patients can make informed choices and notice changes before they occur as they check and record their readings on a regular basis. Finally, SMBG will enable individuals with diabetes to actively manage their health and avoid long-term complications.
Understanding Self-Monitoring of Blood Glucose (SMBG)
Self-Monitoring of Blood Glucose (SMBG) is a type of monitoring that allows those with diabetes to check their sugar levels at home with a glucometer that assists them in managing their condition by making decisions related to diet, physical activity, and drugs. Consistent monitoring will give blood sugar profile, enable treating high or low blood sugar immediately, improve glycemic control, and enhance communication with health care providers.
How SMBG works
A prick of blood is taken (usually a finger) (or occasionally otherwise).
A blood sample is put in a test strip, and a meter will give a reading of blood glucose in a few seconds.
Most meters archive results and can provide trend over time.
Why SMBG is important
Improves glycemic control: With blood glucose monitoring, one can make wise decisions regarding his or her diet, exercise and pharmacology, which results in improved glycemic control.
Assist in recognizing trends: SMBG helps individuals with diabetes and their medical caregivers to know how various factors influence the process of blood glucose levels.
Avoids complications: Long-term diabetes complications may be avoided through regular monitoring, which makes the blood sugar level within the target range.
Issues with hypoglycemia and hyperglycemia: It is vital in diagnosing and managing the dangerous low and high sugar levels promptly.
Facilitates individualized treatment regimens: The data collected can be used to adjust doses of insulin, diet and exercise to produce an individualized treatment regimen.
The Role of Healthcare Providers in SMBG
Self-monitoring of blood glucose (SMBG) depends on healthcare providers, who, through educating patients, ensure they set personalized goals and use data to inform and modify treatment plans. Their role involves initial training, ongoing support, and assisting patients to interpret and make use of SMBG results to regulate diet, exercise, and medication which leads to improved glycemic control and empowerment.
Key roles of healthcare providers in SMBG
Patient education:
Give the first training on how to carry out SMBG properly, the use of meter and ketone test when necessary.
Train patients to understand how to interpret their readings and how food exercise among other factors influences their blood glucose.
Goal setting and personalization:
The partnership with patients to develop personalized SMBG guidelines (frequency and intensity) according to their needs and treatment objectives.
Concur with the reason of SMBG with the patient and record such objectives.
Therapeutic adjustments:
Utilize the SMBG data to make informed and timely decisions on whether to make changes in the areas of medication, lifestyle, and diet.
Help patients to cope with acute conditions such as sickness by monitoring SMBG more often.
Technological advances in glucose monitoring include the development of Continuous Glucose Monitors (CGM) and Flash Glucose Monitors (FGM), which are more convenient and less invasive than traditional finger pricks. Other key advancements are the integration of CGMs with automated insulin delivery (AID) systems, the development of more accurate and smaller sensors, and the exploration of non-invasive and self-powered technologies. These innovations improve glycemic control, reduce hypoglycemia, and provide users with real-time data and alerts.
Final Thoughts
In conclusion, self-monitoring of blood glucose plays a crucial role in achieving better diabetes control and overall well-being. By consistently tracking blood sugar levels, individuals can recognize patterns, make timely adjustments, and work more effectively with their healthcare providers. Regular monitoring not only helps prevent complications but also fosters greater confidence and independence in managing diabetes.
FAQs
What is self-monitoring of blood glucose levels?
Self-monitoring of blood glucose (SMBG) can be a useful tool in the management of diabetes mellitus. Patients with diabetes often measure their blood glucose to detect hypoglycemia and to adjust insulin dose as needed.
What is the 15 minute rule for diabetes?
If your blood sugar is low, follow the 15-15 rule: Have 15 grams of carbs, then wait 15 minutes. Check your blood sugar again. If it’s still less than 70 mg/dL, repeat this process.
What is the 3-hour rule for diabetics? The “three-hour rule” for rapid-acting insulin (aka “Insulin Stacking”) Rapid-acting insulin begins to work about 15 minutes after injection, peaks in about 1 hour, and continues to work for 2 to 4 hours. The three-hour rule prevents “insulin stacking” and a low blood glucose (BG) or hypoglycemia.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
Life with diabetes is much longer than the blood sugar level which can affect emotions, relations and daily activities. Being a way to balance nutrition requirements to preserve social relationships and emotional health, diabetes may change the way people relate with their partners, family, and friends. These difficulties should be comprehended to establish empathy, support, and positive communication. This paper discusses the effects of diabetes on relationships and everyday life and includes information about coping with them in a resilient and positive way.
Understanding Diabetes and Its Challenges
Diabetes is a chronic condition where the body has high blood sugar because it doesn’t produce enough insulin or can’t effectively use the insulin it makes. This can damage organs and lead to complications like heart disease, vision loss, and kidney disease. Challenges include managing the disease through lifestyle changes, medication, and blood sugar monitoring, as well as overcoming healthcare system inefficiencies and improving patient-provider communication.
What is diabetes?
Core issue: Diabetes is the inability of your body to transport glucose (sugar) in blood to your cells to provide energy.
Role of insulin: Glucose gets into cells with the help of insulin. In diabetes, insulin is either insufficient or is not utilized normally.
Result: The glucose accumulates in the blood resulting into high blood sugar (hyperglycemia).
Health risks: This may in the long term severely harm the nerves, blood vessels, eyes, kidneys and heart.
Common challenges
Managing the condition: This entails the multi-dimensional method of medication, blood glucose, and carbohydrate counting.
Lifestyle changes: Individuals with diabetes have to adopt healthy lifestyles that include healthy weight, balanced diet and regular exercise.
Healthcare access: The coverage of treatment has disparities with less resources in low and middle-income countries.
Communication between patients and providers: Certain patients complain that medical practitioners are not empathetic, disrespect them, or do not involve them in treatment decisions.
Health system inefficiency: The barriers to effective diabetes management may include ineffective systems and caregivers.
Emotional and Psychological Impact
The emotional and psychological effects of diabetes are considerable, such as distress, anxiety, and depression, which are associated with worse health results and complications. Self-management of this condition can become frustrating, angry, and burnout-inducing. These psychological effects are vital to deal with to improve disease control and quality life.
Common emotional and psychological effects
Diabetes distress: A unique emotional burden related to the daily burden of living with the disease.
Depression: It is more prevalent among individuals with diabetes and may cause deteriorated self-management, health, and complications.
Anxiety: There is a lot of worry and fear, which are often about getting the condition under control, such as the fear of hypoglycemia (hypo).
Stress: It is possible to influence the level of blood sugar directly, because stress hormones may lead to sudden increases or decreases.
Other feelings: Individuals can also feel angry, tired, frustrated, sad, guilty, and burned.
The Effect on Family and Romantic Relationships
Diabetes influences relationships because it is a unifying risk factor between partners and families, it affects emotions and health behaviors. Positively, good family and romantic support is connected to improved management and treatment compliance. Nevertheless, bad dynamics, poor communication, or stress may impair the health outcomes of a patient and the quality of the relationship itself.
How Diabetes affects family and romantic relationships
Shared health risks: A study conducted by the National Institutes of Health (NIH) shows that people having diabetes as partners increase the risk of developing diabetes in their partners because of shared lifestyle, biological, and assortative mating of other risk factors such as BMI and blood pressure.
Emotional and psychological stress: The continual care of diabetes may result in anger, frustration, worry, isolation, and stress in the diabetic, which can cause a strain on the relationship.
Effects on relationship dynamics: According to research on ResearchGate, controlling/overprotective behavior by one of the partners may be reported as negative, whereas invisible support can be more beneficial in enhancing health outcomes.
Shared lifestyle influence: Partners tend to have poor lifestyle habits such as poor diet and lack of exercise, which can be a source of conflict, or a common issue that must be resolved collectively.
How family and relationships can affect diabetes management
Positive effects:
Greater compliance: Social and familial support has been mostly associated with increased adherence to treatment and management plans.
Better outcomes: Favorable family functioning is related to enhanced self-care practices and enhanced glycemic control.
Behavior changes: In cases where one partner undergoes favorable changes in lifestyle, the other partner is likely to do the same.
Negative effects:
Poor outcomes: A low-quality marriage may worsen the results of diabetes and patient management capabilities.
Communication breakdown: Ineffective communication about the disease may result in misunderstanding, frustration and reduced life quality of both partners.
Effective strategies:
Outcome: Involving family members in diabetes education may result in healthier family behaviors and encourage patient self-management.
Couples counseling: A counselor can assist couples to communicate more effectively and make health a common objective which may result in a more organized way of addressing diabetes.
If you have diabetes: Support groups Support groups can also be helpful in minimizing feelings of isolation and offer helpful advice.
Managing Daily Life with Diabetes
Daily living with diabetes requires a regular regimen of healthy eating, exercise, and glucose monitoring, prescribed medication and regulation of stress. Healthy diet involves paying attention to portion size and consuming nutritious foods and reducing sugar, salt, and unhealthy fats. Exercising on a regular basis may incorporate a balance of aerobic and strength-training exercises and regular majoring can help you know how your body reacts to food and activities.
Diet and nutrition
· Use the plate rule: Make half of your plate with non-starchy veggies, a quarter with lean protein, and the last quarter with healthy carbohydrates such as whole grains or fruit.
· Selectively restrict poor foods: Eat less sweetened beverages, processed items, and high saturated fat foods. Instead of soda, take water and fruit because it is a sweet treat.
· Controlling portions: Pay attention to portions. Use measuring cups or use everyday items such as a deck of cards (meat) or fist (pasta) to estimate portions of food. Keep Away Dehydration: keep hydrated by drinking lots of water throughout the day.
Monitor your salt consumption: Have salt in moderation of approximately 6 grams (one teaspoon) per day because a lot of the packaged foods have concealed salt. Prepare your own meals to have healthier control of salt.10 tips for healthy eating with diabetes
Physical activity
Goal: 150 each week: At least 150 minutes of an activity of moderate intensity (e.g. brisk walking) at least once a week.
Regularly test blood sugar: You must check your blood sugar level to know what causes it to rise or fall. This knowledge is essential in making changes to your treatment plan.
Take medicine: This is because when you are not feeling well, it is important to take all medications as required whether you feel well or not.
Balance food and medicine: Take care that you have a balance between food and medication. Excess food may result in elevated blood sugar whereas insufficient food may result in excessively low blood sugar (hypoglycemia).
Stress and mental health
Accept stress: Recognize that being a diabetic can be a stressful experience, and it is only natural to at times feel overwhelmed, angry, or burned out.
Improve coping skills: Learn to deal with stress. In case you are having difficulties, consult your healthcare specialist.
Sleep well: It is recommended to get a good sleep of about 7 to 8 hours a day as it is likely to improve your mood, energy and blood glucose levels.
Final Thoughts
Diabetes covers a lot of life such as personal relationships, daily life but it does not need to restrict the happiness or fulfillment of life. Knowledge, openness, and regular self-care help people and their loved ones to develop stronger relationships and provide a conducive environment. Through patience and optimism toward diabetes, one can have a normal and fulfilling life.
FAQs
How does diabetes affect relationships?
What happens to mood and relationships with diabetes? The process of coping with diabetes can be stressful, and the change in blood sugar levels can also serve as a cause of mood changes. Such factors can put a burden on relationships. Diabetes affects the body by utilizing blood glucose.
How does diabetes impact someone emotionally?
Individuals with diabetes are prone to depression 2-3 times more often than those without diabetes. Only a quarter to half of diabetic individuals with depression are diagnosed and treated. Treatment, however, therapy or both, is often very successful. And untreated, depression tends not to improve, but to deteriorate.
Does diabetes cause anger issues?
Unchecked blood sugar directly influences your emotions; behaviors changes and mood swings occur. Once diagnosed with any chronic illness such as diabetes, a broad range of feelings will also be unsurprising to you: denial and anger, stress, grief, and sadness.
Dr. Ahmad Shahzad Founder | Lyallpur Diabetes Foundation Consultant Diabetologist | Educator | Advocate for Preventive Care
Diabetes is a condition that requires continuous emotional, physical, and social support to live with it. This journey is easier and more rewarding when one can relate with others who have had similar experiences. Diabetes peer support groups provide a secure and understanding environment where individuals can share knowledge. They go through hardships and celebrate victories. These groups are very crucial in enabling individuals to take up control of their health and enhance their quality of life.
Understanding Peer Support Groups
Peer support groups include meetings of people with common experiences to offer mutual aid, emotional support, and understanding. These organizations are rooted in values of respect, collective responsibility, and empathy. It can be a significant asset in dealing with mental illnesses, addiction, or other life problems. Peer support groups provide an opportunity to exchange stories. They can comfort you in the fact that you are not the only one and assist in self-development and recovery.
Key characteristics of peer support groups
Shared experience:
The members have been through such hardships as mental illnesses or alcoholism. It has established a background of understanding and empathy.
Mutual aid:
The first one is to support each other with experiences, to be empathetic, compassionate, and encouraging.
Supportive environment:
Groups provide a secure environment where members exchange their experiences, achievements, and challenges freely.
Beyond clinical models:
Peer support is not grounded in the standard psychiatric constructs but in the empathy of another with emotional and mental suffering.
Focus on recovery and wellness:
Individuals can teach each other, be role models, and promote their recovery and wellness.
Emotional and Psychological Benefits
These groups also offer empowerment, hope, and the development of new coping skills. It provides a supportive environment to talk openly, learn from others, and gain a sense of control.
Emotional benefits
Less isolation: You feel less alone when you contact other people who have gone through the same thing.
Shared understanding: The sense of being very understood by people who have gone through it is an effective source of comfort.
Validation: When others say that their experiences are real and they should not be ashamed of it. It can be a huge relief and can diminish feelings of guilt or alienation.
Hope and empowerment: Seeing other people who have survived the same difficulties can grant hope and a feeling of control, empowerment, and motivation.
Psychological benefits
Better coping abilities: Groups offer a safe environment where it is possible to share feelings and learn new coping strategies through peers.
More self-awareness: Sharing feelings aloud will help them become more real. It result in more awareness and knowledge of what you are feeling.
Knowledge and practical feedback: Members can get knowledge about their condition, get feedback on treatment options, and find new resources in others.
Sense of purpose: These groups may assist individuals in gaining a sense of purpose that serves as a safeguard against life challenges and long-term objectives.
Educational and Practical Support
They provide a space to learn other lived experiences and skills educationally, and in practice, emotional support, a sense of community, and a resource and strategy sharing place. This personal empowerment enables people to gain confidence and self-management skills, which result in improved performance.
Educational support
Sharing knowledge and skills: Members can learn about each other by sharing knowledge, strategies and information about the experiences they share.
Self-efficacy: With the help of peer encouragement, people will develop self-efficacy, having confidence in their ability to cope with their own health and life issues.
Normalizing experiences: The groups are safe spaces to share difficulties and responses, and this makes members realize that their experiences are normal and legitimate.
Collaborative learning: Peer support may serve as a type of collaborative teaching-learning, where members learn and teach one another.
Practical support
Practical support: Members may offer physical support, including resource sharing or advice on system and service navigation.
Developing strength: The reliability of peer support and encouragement assists in developing individual and community strength.
Empowerment and control: Peer support enables people to define their health and well-being and gain greater control over their life.
Technology can offer peer support via online forums, applications and social media groups to individuals living with conditions such as diabetes, amongst the advantages are accessibility, anonymity and global community. Nevertheless, consumers should give privacy priority and ensure that they verify online sources to avoid misinformation and harassment.
Examples of technology in diabetes peer support
Online forums:
Specialized websites, such as the American Diabetes Association (ADA) Community and Diabetes Link, can be used to discuss and ask questions and share experiences.
Mobile apps:
Applications such as the Diabetes forum connect huge groups of people right on the phone of the user.
Social media groups:
Although they are not so organized, these groups give a feeling of community and allow peer-to-peer interaction.
Benefits of virtual support
Accessibility:
Anytime, anyplace support is offered, and this is essential because people with chronic conditions might not have good mobility or access to face-to-face groups.
Anonymity:
It allows users to open and ask some sensitive questions without worrying about being judged, which can be a big plus to individuals who are shy to do the same in a real-life context.
Global reach:
Geographical boundaries are broken as people can connect with other people worldwide who have been experiencing similar things.
Risks and precautions
Privacy:
Care must be taken when sharing personal issues about health on the internet. Users ought to know how their data is utilized and what the privacy settings of their accounts or applications are.
Credible sources:
The data published in Web forums may be different in its accuracy. Before falling into misinformation, it is critical to confirm information with valid sources and medical practitioners to prevent any harm and to make sure that any recommendations are safe and correct.
How to Join or Start a Diabetes Peer Support Group
In order to become a member of a diabetes peer support group, Google identify local or national organizations or use social media sites to find groups. To form a group, refer to a diabetes organization about the way to start and where to locate resources. The two choices will enable you to locate a community where you can experience and get support.
How to join a diabetes support group
Search online: Enter search engines with diabetes support group near me or online diabetes support group to locate both local and online.
Look at national/local organizations: A variety of diabetes organizations, such as Diabetes Australia, Diabetes Canada, and Breakthrough T1D, have online community, support program, and resources.
Use social media: Find closed or private groups on websites such as Facebook to find people with similar experiences in private.
Contact your health provider: Have your doctor or a diabetes educator know of any local support group or be referred to one.
How to start a diabetes support group
Link to a local organization: Contact your state or national diabetes organization to get ideas and resources to start a new group.
Find professional involvement: You can also explore interest in other existing networks, which can also assist you to establish ties and incorporate them in a bigger care plan.
Find resources: Look for resources and examples of how other organizations have set up their own groups, such as those documented on the HSE website.
Plan and promote: Once you have a framework, you can begin to promote the group to your community and gather interested members.
Final Thoughts
To sum up, peer support groups are invaluably valuable to individuals with diabetes since they offer emotional support, learning, and encouragement to adhere to healthy lifestyles. They also fill the disconnects between medical services and normal life, making people have more confidence and encouragement to live with the condition. Physically or virtually, being part of a diabetes peer group can generate a significant impact on addressing physical and emotional health.
FAQs
How to find diabetic friends?
Check to see whether there is a diabetes organization chapter in your area. Locate your local chapter and ask them whether they have events on their webpage. You can also call them to inquire whether they have other contacts with T1D.
What does a diabetes support group do?
We have a diabetes support group which is an emotional and resource-based peer connection group of individuals and caregivers that manage diabetes and pre-diabetes.
What is peer support for type 2 diabetes?
Peer support in diabetes self-management allows patients to engage in mutual knowledge-sharing, collaborative problem-solving, and emotional support for the stresses of dealing with type 2 diabetes.
What is the National Programme for Diabetes?
To prevent and control major NCDs, Government of India has implemented the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) in all States across the country with the focus on strengthening of infrastructure, development of human resource.
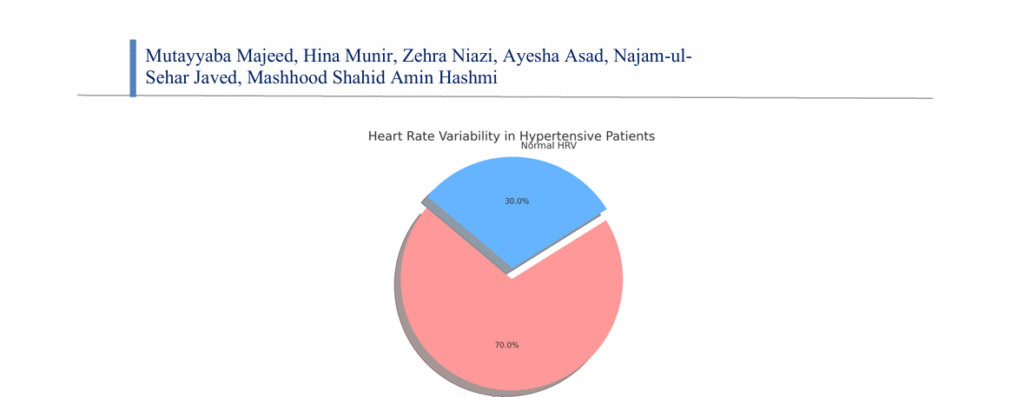
*1Assistant Professor, Department of Physiology, Independent Medical College, Faisalabad. 2Assistant Professor, Department of Physiology, AJK Medical College, Muzaffarabad Email ID: hinatahir1126@gmail.com 3Assistant Professor, Department of Physiology University Medical & Dental College, Faisalabad Email ID: Zehra.niazi@tuf.edu.pk 4Associate Professor, Department of Anatomy Akhtar Saeed Medical College, Rawalpindi Email ID: ashi.asadd11@gmail.com 5PGR, FCPS, Department of Physiology Rawalpindi Medical University, Rawalpindi Email ID: najamjaved25@gmail.com 6Senior Registrar, Cardiac Surgery, Rawal General and Dental Hospital, Rawalpindi. Email ID: mashhood911@yahoo.com *Corresponding Author: Mutayyaba Majeed, Email ID: mutayyaba.asad@gmail.com Cite this paper as: Mutayyaba Majeed, Hina Munir, Zehra Niazi, Ayesha Asad, Najam-ul-Sehar Javed, Mashhood Shahid Amin Hashmi, (2025) Autonomic Nervous System Dysfunction In Hypertensive Patients: A Heart Rate Variability (HRV) Analysis. Journal of Neonatal Surgery, 14,(31s) 1075-1080.
ABSTRACT
Background: Hypertension, the most prevalent cardiovascular disorder, significantly escalates the risks of stroke, myocardial infarction, and renal diseases. It is believed that an imbalance of the autonomic nervous system (ANS), particularly heightened sympathetic tone and reduced parasympathetic regulation, underlies its pathogenesis. One of the non invasive approaches to study the ANS is the analysis of heart rate variability (HRV). Objectives: To evaluate autonomic nervous system impairment in hypertensive patients and to evaluate the heart rate variability (HRV); then compare the findings with normal subjects (normotensive) to establish the statistical significance. Study design: Cross-sectional comparative study. Place and duration of study: July 2024 to December 2024, Independent University Hospital, Faisalabad. Methods: The study was carried out on 100 patients with hypertension, and 100 age matched normotensive controls. A 5 minute ECG and measurement of HRV were made during resting state. Parameters in time-domain and in frequency-domain were analyzed. Descriptive statistics were determined with mean and standard deviation and independent t-tests in order to determine the differences between groups. All comparisons were measured to be statistically important at p < 0.05. Results: One hundred hypertensive patients (mean age: 54.22 9.6 years) and one hundred normotensive controls (mean age:53.72 8.9 years; p = 0.67) were studied. There are also lower HRV indexes; SDNN or Standard Deviation of Normal-to Normal intervals, a key measure of HRV (36.4 12.3 ms vs. 48.7 14.1 ms, p < 0.001) and RMSSD or Root Mean Square of successive Differences (21.1 9.2 ms vs. 31.5 10.7 ms, p < 0.001) in hypertensive subjects. Frequency-domain also indicated lower parasympathetic (HF) and greater sympathetic (LF/HF ratio) modulation comparisons of hypertensive compared to controls (p < 0.05). These results confirm the existence of autonomic alteration among hypertensive patients. Conclusion: A major dysfunction of the autonomic mechanisms related to a low heart rate variability is seen in hypertensive patients. The results show reduced activity of parasympathetic system and the increased sympathetic dominance. The HRV analysis is useful and non-invasive to determine autonomic balance in hypertensive people and can be to help in early detection and risk stratification. The regular use of HRV in the chain of hypertension treatment and management would increase patient-centered approaches.
INTRODUCTION
Autonomic dysfunction is usually linked to hypertension, a major cause of morbidity and mortality related to the cardiovascular system all over the world. ANS is considered a key regulator of the heart rate and blood pressure, and the imbalance of this system may cause a serious impact on the condition of cardiovascular system [1]. One exceptionally good measure of ANS and its variability is heart rate variability (HRV) or the difference in time between successive heart beats. These data on the HRV analysis yield important information about autonomic control of cardiovascular functioning and study the equilibrium between the sympathetic and parasympathetic divisions of the Aspin in the hypertensive patients, the deregulation of this autonomic control is often associated with the deterioration of the preservation of HRV, and it is associated with cardiovascular risks and poor prognosis [2]. Sympathetic nervous system (SNS) activity is usually excessive leading to elevation of heart rate and blood pressure and parasympathetic nervous system activity is suppressed and it takes part in intensifying the hypertension and cardiovascular disease (CVD) situation. It has been demonstrated in many works that a low HRV leads to increased probability of developing cardiovascular incidents like myocardial infarction, stroke and arrhythmias and therefore analysis of HRV makes a significant contribution in the care of hypertensive patients. Studies of the HRV in hypertensive patients have found that decreased HRV could be a prognostic marker of unfavorable cardiovascular events [3]. Besides, enhancement of HRV by making lifestyle changes (e.g. physical activity and stress reduction) as well as pharmacological conditions (e.g. beta-blockers, ACE inhibitors) can result in a more favorable blood pressure and decreased risk of CVD. On the one hand, the strong correlation between HRV and hypertension is established; on the other hand, further study is required to identify some of the definite mechanisms leading to autonomic dysfunction in patients with hypertension and the long-term effects on cardiovascular health [4,5]. In our paper, we are going to examine HRV in patients with essential hypertension by means of the time-domain analysis, frequency-domain and non-linear analysis [6]. We hope that our study into the relationship between HRV and hypertension will contribute to increased insight into the importance of an autonomic dysfunction in hypertensive patients and its possible impact on the definition of the treatment strategy used to support cardiovascular outcomes [7].
METHODS
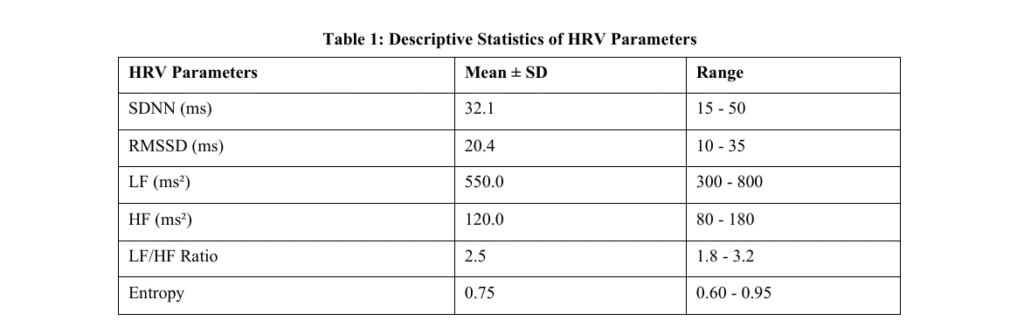
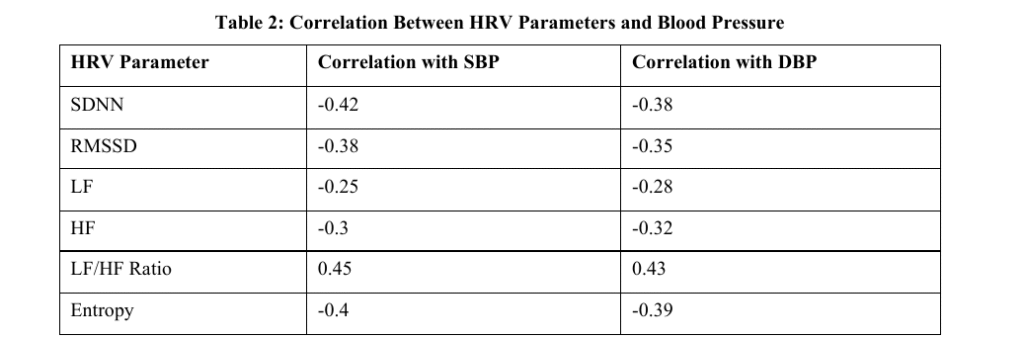
This was a cross-sectional study which included 100 patients with hypertension who had a diagnosis of essential hypertension. The participants were chosen in a tertiary care hospital and undertaken thorough cardiovascular examinations. HRV recordings were conducted with the help of a 24-hour Halter monitor. The SDNN, RMSSD, LF, HF and LF/HF ratios were computed in the time- and frequency-domain, respectively. Analysis Non-linear analysis was conducted using Poincare plot, the entropy. The analysis of data was performed by SPSS 24.0 and different levels of hypertension and HRV parameters were compared. Study design: Cross-sectional comparative study. Place and duration of study: January 2024 to July 2024, Independent University Hospital, Faisalabad. Ethical Approval Statement: The study received authorization by the institutional review board. Informed consent was taken on paper and all participants gave their written consent. Inclusion Criteria: The study was based on patients with essential hypertension who were aged between 30 to 70 years. Exclusion Criteria: The patients that had secondary hypertension, arrhythmia, or had a known cardiovascular disease were not included in the study. Data Collection: To measure intervals of heart beats, data were obtained by attachment of a 24-hour Halter monitor. Medical records were used to collect clinical data in terms of age, gender, and medical history. Statistical Analysis: The SPSS version 24.0 was used in the analysis of data. Comparisons of the parameters of HRV were based on descriptive statistics, independent t-tests, and ANOVA of the hypertensive subgroups. Results: The study included one hundred hypertensive patients, having an average age of 55.3 +/ 8.2 years. Analysis of HRV indicated that the mean SDNN of hypertensive patients was much lower than that of healthy participants (mean = 32.1 a 10.5 ms, pHs < 0.05) and the same was applicable to RMSSD (mean = 20.4 a 5.6 ms, pHs < 0.05). The analysis in the frequency domain indicated lower high-frequency components (HF; mean = 550 +/- 120 ms 2) with the higher ratio of LF/HF (mean =2.5 +/- 0.9), which is symptoms of sympathetic dominance. Compared with hypertensive patients, non-linear analysis also showed that the entropy levels were also lower indicating that there was less complexity in the heart rates of hypertensive patients. These results were similar between those patients with mild hypertension and severe hypertension. Moreover, the parameters of HRV were negatively related to systolic blood pressure and diastolic blood pressure (r = -0.42 and r = -0.38, p < 0.01, respectively). The findings indicate that low HRV is linked with the extremity of hypertension and could be a causative marker of cardiovascular risks among these individuals.
DISCUSSION
High blood pressure is a major risk factor of cardiovascular diseases and may be accompanied by dysfunction of the autonomic nervous system (ANS). Heart rate and blood pressure is the autonomic control that is necessary to support cardiovascular homeostasis [8]. The study objective was to assess the heart rate variability (HRV) among patients with hypertension to gain an indicator of autonomic dysfunction. The results of our investigations demonstrate the presence of notable decreases in the HRV of hypertensive patients as an indicator in comparison to the healthy control group and the direct correlation of the parameters of the heart rate variability and the values of the blood pressure. These findings correlate with a number of studies, which have addressed the correlation between HRV and hypertension. Relation of hypertension and low HRV has been documented well in the literature [9, 10]. A recent study by Srinivasan et al. (2012) showed that patients with essential hypertension had markedly reduced HRV (accompanied by significant decrease of both the time- and frequency-domain parameters) [11]. Their results implied that the autonomic dysfunction that prevailed among these individuals is mainly attributed to the factors of sympathetic hyper activity and parasympathetic withdrawal [12]. These findings are backed by our study, as well, with decreased SDNN, RMSSD components, and HF component, demonstrating the lower rate of the parasympathetic activity, and higher sympathetic tone, in hypertensive patients. Regarding the analysis in the frequency domain, our study identified that the ratio LF/HF was higher among the patients with hypertension, which shows a shift in the dominance to sympathetic [13]. This concurs with the findings of Mania et al. (2007) who indicated that the increased LF/HF ratio is a prevalent condition among patients who are hypertensive and that such practice could also be used to predict poor cardiovascular outcomes [14]. In the same line, Shaffer and Ginsberg (2017) argued that LF/HF ratio is a sensitive indicator to evaluate roles of sympathetic and parasympathetic branches of ANS especially in relation to cardiovascular diseases such as hypertension [15]. Also consistent with our study is the work of Kuok et al. (2009) who performed an analysis on the autonomic dysfunction in a group of hypertensive subjects and concluded that the lower the HRV the poorer the prognosis and the higher the risk of cardiovascular morbidity and mortality, namely arrhythmias and heart failure occurred. Muller et al. (2011) also showed that lower HRV was associated with major adverse cardiovascular events (MACE) in patients with chronic hypertension enhancing clinical relevance of HRV as the indicator of cardiovascularrisk [16].It has been suggested that in hypertensive individuals, the decrease in HRV is a result of long-term changes in sympathetic and parasympathetic tone [16]. The chronic hypertension may cause structural and functional alterations of the autonomic centers of brain and brainstem, as well as hypothalamus. The changes can lead to dysbalance between over activity of the sympathetic nervous system and withdrawal of the parasympathetic nervous, as observed by Thayer et al. (2010), who proposed that any disorder in the autonomic nervous system is main determinative factor in the path physiology of hypertension and other medical states of the heart and circulatory system [17,18].Also reported, HRV turns out to be independent predictor of complications associated with hypertension. In another study by Liao et al. (1996), the risk of developing of coronary artery diseases in hypertensive patients was associated with lower HRV, despite the impact of the usual risk factors like age, cholesterol level and smoking habits. It is evidence in the hypothesis that HRV can be applied as an early risk stratification tool in hypertensive individuals.
CONCLUSION
This study emphasizes that there was a large minimization of heart rate variability (HRV) in hypertensive people that shows failure of some measure on autonomy. HRV may become a useful instrument in evaluation of cardiovascular risk and evaluation of treatment outcomes in hypertension. Better HRV can lead to the improved blood pressure levels and lower cardiovascular risks.
LIMITATIONS
The cross-sectional design of this study does not allow determining the causation between lowered HRV and hypertension. Also, sample size and absence of long term follow up can limit the generalisablility of discovery. Medication and lifestyle were other factors that were not exclusively controlled, and they may affect HRV results. Recommendations Future studies must focus on to investigate how HRV can influence hypertension development long term and whether or not the interventions are successful in rescuing the situation where the autonomic function is failing. Examination of mechanisms in different forms of hypertension with the inclusion of genetic and environmental factors may contribute to a better understanding and provision of a more individual approach to treatment.
ABBREVIATIONS
HRV – Heart Rate Variability
ANS – Autonomic Nervous System
SBP – Systolic Blood Pressure
DBP – Diastolic Blood Pressure
LF – Low-Frequency
HF – High-Frequency
SDNN – Standard Deviation of Normal-to-Normal intervals
RMSSD – Root Mean Square of Successive Differences
MACE – Major Adverse Cardiovascular Events
ESC – European Society of Cardiology
ESH – European Society of Hypertension Disclaimer: Nil Conflict of Interest: Nil Funding Disclosure: Nil Authors Contribution Concept & Design of Study: Mutayyaba Majeed, Zehra Niazi, , Mashhood Shahid Amin Hashmi Drafting: Hina Munir, Ayesha Asad Data Analysis: Hina Munir, Zehra Niazi Critical Review: Mutayyaba Majeed, Najam-ul-Sehar Javed Final Approval of version: Mutayyaba Majeed, Hina Munir, , Mashhood Shahid Amin Hashmi
REFERENCES
[1] Arslan D, Ünal Çevik I. Interactions between the painful disorders and the autonomic nervous system. Agri :Agri (Algoloji) Dernegi’nin Yayin organidir = The journal of the Turkish Society of Algology. 2022;34(3):155
[2] Bellocchi C, Carandina A, Montinaro B, Targetti E, Furlan L, Rodrigues GD, et al. The Interplay between Autonomic Nervous System and Inflammation across Systemic Autoimmune Diseases. International journal of molecular sciences. 2022;23(5). [3] Benarroch EE. Physiology and Pathophysiology of the Autonomic Nervous System. Continuum (Minneapolis, Minn). 2020;26(1):12-24. [4] Brazdil V, Kala P, Hudec M, Poloczek M, Kanovsky J, Stipal R, et al. The role of central autonomic nervous system dysfunction in Takotsubo syndrome: a systematic review. Clinical autonomic research : official journal of the Clinical Autonomic Research Society. 2022;32(1):9-17. [5] Camilleri M. Gastrointestinal motility disorders in neurologic disease. The Journal of clinical investigation. 2021;131(4). [6] Chen Z, Li G, Liu J. Autonomic dysfunction in Parkinson’s disease: Implications for pathophysiology, diagnosis, and treatment. Neurobiology of disease. 2020;134:104700. [7] Franco C, Previate C, Trombini AB, Miranda RA, Barella LF, Saavedra LPJ, et al. Metformin Improves Autonomic Nervous System Imbalance and Metabolic Dysfunction in Monosodium L-Glutamate-Treated Rats. Frontiers in endocrinology. 2021;12:660793. [8] Iser C, Arca K. Headache and Autonomic Dysfunction: a Review. Current neurology and neuroscience reports. 2022;22(10):625-34. [9] Kaur D, Tiwana H, Stino A, Sandroni P. Autonomic neuropathies. Muscle & nerve. 2021;63(1):10-21. [10] Khemani P, Mehdirad AA. Cardiovascular Disorders Mediated by Autonomic Nervous System Dysfunction. Cardiology in review. 2020;28(2):65-72. [11] Kiryachkov YY, Bosenko SA, Muslimov BG, Petrova MV. Dysfunction of the Autonomic Nervous System and its Role in the Pathogenesis of Septic Critical Illness (Review). Sovremennye tekhnologii v meditsine. 2021;12(4):106-16.
[12] Kłysz B, Bembenek J, Skowrońska M, Członkowska A, Kurkowska-Jastrzębska I. Autonomic nervous systemdysfunction in Wilson’s disease – A systematic literature review. Autonomic neuroscience : basic & clinical. 2021;236:102890. [13] Lefaucheur JP. Assessment of autonomic nervous system dysfunction associated with peripheral neuropathies in the context of clinical neurophysiology practice. Neurophysiologie clinique = Clinical neurophysiology. 2023;53(2):102858. [14] Mohammadian M, Golchoobian R. Potential autonomic nervous system dysfunction in COVID-19 patients detected by heart rate variability is a sign of SARS-CoV-2 neurotropic features. Molecular biology reports. 2022;49(8):8131-7. [15] Piętak PA, Rechberger T. Overactive bladder as a dysfunction of the autonomic nervous system – A narrative review. European journal of obstetrics, gynecology, and reproductive biology. 2022;271:102-7. [16] Scott RA, Rabinstein AA. Paroxysmal Sympathetic Hyperactivity. Seminars in neurology. 2020;40(5):485-91. [17] Silvani A. Autonomic nervous system dysfunction in narcolepsy type 1: time to move forward to the next level? Clinical autonomic research : official journal of the Clinical Autonomic Research Society. 2020;30(6):501-2. [18] Urbini N, Siciliano L, Olivito G, Leggio M. Unveiling the role of cerebellar alterations in the autonomic nervous system: a systematic review of autonomic dysfunction in spinocerebellar ataxias. Journal of neurology. 2023;270(12):5756-72.